

With the acceleration of global population aging, diabetic kidney disease (DKD) is gradually becoming a “silent killer” that threatens the health of the elderly. According to the Lancet Global Burden of Disease study 2023, there have been 788 million chronic kidney disease patients aged 20 years and older worldwide, of which diabetes is the leading cause of end-stage renal disease. Driven by aging, the incidence, prevalence and disease burden of diabetic kidney disease are on the rise, posing a serious challenge to the public health system and social and economic development.
1. Bidirectional association between aging and diabetic nephropathy
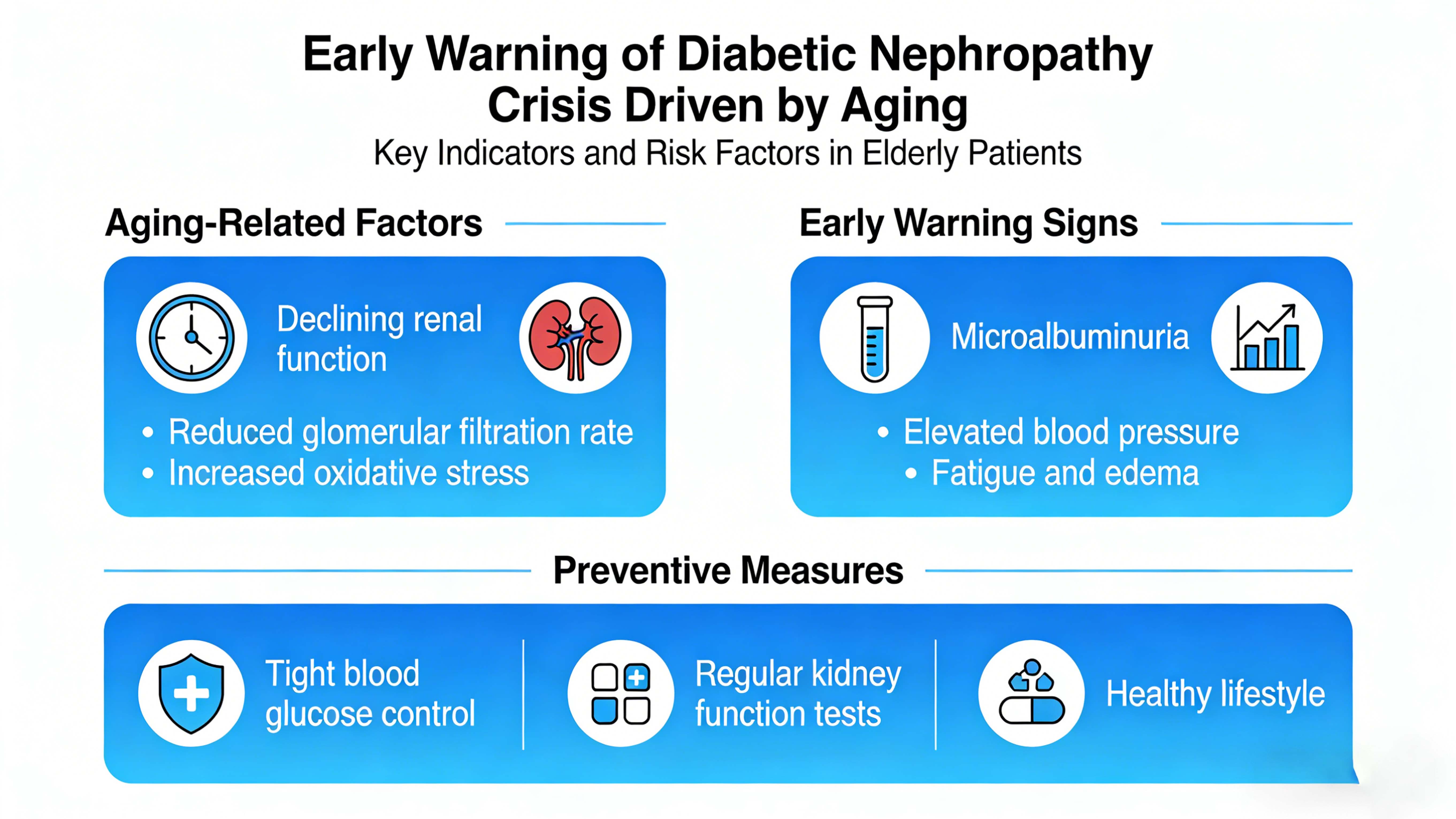
There are complex bidirectional associations between aging and diabetic kidney disease:
01 The additive effect of physiological decline: with aging, the physiological function of the kidney gradually declines, the glomerular filtration rate (GFR) declines at a rate of about 0.75 to 1.0ml/min per year, and the self-repair ability of the kidney is also weakened. At the same time, insulin resistance is increased, islet β cell function is decreased, and the risk of diabetes is significantly increased in the elderly. The additive effect of this physiological decline and diabetes makes elderly diabetic patients more susceptible to kidney injury.
02 Synergistic damage of comorbidities: Elderly patients with diabetes mellitus are often combined with hypertension, hyperlipidemia, cardiovascular disease and other chronic diseases, which can synergistically impair kidney function. The study showed that the risk of diabetic nephropathy in diabetic patients with hypertension was 2.3 times that in diabetic patients without hypertension. The risk was 4.1 times higher in patients with hypertension and hyperlipidemia.
Increased risk of drug-induced kidney injury: Elderly patients often need to take multiple drugs at the same time, and some hypoglycemic drugs, antihypertensive drugs, non-steroidal anti-inflammatory drugs have certain nephrotoxicity. In addition, elderly patients have a decreased ability to metabolize drugs and a prolonged half-life in the body, further increasing the risk of drug-induced kidney injury.
04 The impact of cognitive decline: Some elderly patients have cognitive decline, which may lead to irregular blood glucose monitoring, non-compliance with medication and other problems, thus affecting the effect of blood glucose control and accelerating the progress of diabetic nephropathy. blood glucose kit
2. The prevalence and trend of diabetic nephropathy under the background of aging
01 The incidence continues to rise: according to the Global Burden of Disease (GBD) 2021 data, the age-standardized incidence rate (ASIR) of type 2 diabete-related chronic kidney disease in the world increased by 1.928% per year from 1990 to 2021, and the growth rate in China was as high as 2.682% per year. In the elderly population over 65 years old, the incidence of diabetic nephropathy has reached 30%-50%, which is 2-3 times that of young and middle-aged patients.
02 Significantly increased prevalence: As the population ages and the prevalence of diabetes increases, the prevalence of diabetic nephropathy has also shown a significant increase. In 2023, the number of Chinese adults with chronic kidney disease has reached 152 million, and about 30% of them are caused by diabetes. In elderly patients with diabetes, the prevalence of diabetic nephropathy is as high as 40%-60%.
The increasing burden of disease: diabetic nephropathy not only seriously affects the quality of life of patients, but also brings heavy economic burden. According to statistics, the annual average medical cost of patients with end-stage renal disease is as high as 100,000-150,000 yuan, and the medical cost of elderly patients is 1.5-2 times of young and middle-aged patients due to more complications and poor physical conditions. In addition, diabetic nephropathy can also lead to the loss of labor ability of patients and bring indirect economic losses to families and society.
The future trend is not optimistic: According to the Bayesian age-period-cohort (BAPC) model, the global and Chinese burden of type 2 diabetis-related chronic kidney disease will continue to increase in the next decade. With the further aggravation of population aging, the number of elderly diabetic patients will continue to increase, and the prevention and control situation of diabetic nephropathy will become more severe.
3. Early warning and screening strategies for diabetic nephropathy under the background of aging
Early warning and screening are the key to delaying the progression of diabetic nephropathy and reducing the burden of disease:
Identification of high-risk groups: Elderly diabetic patients, especially those with hypertension, hyperlipidemia, cardiovascular disease, obesity and other risk factors, are at high risk of diabetic nephropathy. In addition, elderly patients with family history of diabetes, long-term poor blood glucose control, smoking and alcohol abuse should also be listed as key screening objects.
02 Early screening indicators: urinary albumin/creatinine ratio (UACR) : is the first choice for early screening of diabetic nephropathy, it is recommended to test 1-2 times a year. When UACR≥30mg/g, early renal injury is suggested.
Glomerular filtration rate (eGFR) : serum creatinine, age, gender and other factors can be calculated, it is recommended to test once a year. When eGFR<60ml/min/1.73m², renal function decreased.
04 Serum cystatin C is a sensitive indicator of glomerular filtration function, which is not affected by age, gender, muscle mass and other factors. It can be used as a supplementary indicator of eGFR.
05 Renal injury markers, such as neutrophil gelatinase-associated lipocalin (NGAL) and kidney injury molecule-1 (KIM-1), can detect renal injury earlier, but have not been widely used in clinical practice.
06 Screening frequency: UACR and eGFR are recommended to be screened once a year for elderly diabetic patients without renal damage. Screening every 3 to 6 months is recommended for patients with early kidney injury. For patients with established diabetic nephropathy, the frequency of screening should be increased according to the severity of the disease.
Screening pathway optimization: diversified screening pathways should be established, including hospital outpatient screening, community screening, home self-monitoring, etc. At the same time, Internet technology should be used to carry out remote screening and follow-up to improve the coverage and convenience of screening. blood glucose machine
4. Comprehensive management strategies for diabetic nephropathy under the background of aging
01 Glycemic control: Tight glycemic control is fundamental to delaying the progression of diabetic nephropathy. For elderly diabetic patients, individualized glycemic control goals should be established according to age, health status, comorbidities and other factors. In general, glycosylated hemoglobin (HbA1c) should be <7% in patients younger than 65 years who are in good health; HbA1c can be relaxed to <7.5%-8.0% in patients over 65 years of age, in poor health, or with severe complications. In the selection of hypoglycemic drugs, priority should be given to drugs that have less effect on the kidney, such as metformin, GLP-1 receptor agonists, SGLT2 inhibitors, etc.
02 Blood pressure control: Hypertension is an important risk factor for the progression of diabetic nephropathy, and strict blood pressure control can significantly delay the progression of renal injury. For elderly patients with diabetes, blood pressure should be controlled below 140/90 MMHG. For patients with proteinuria, blood pressure should be controlled below 130/80 MMHG. In the selection of antihypertensive drugs, ACEI or ARB drugs are the first choice, these drugs can not only reduce blood pressure, but also reduce urinary protein and protect renal function.
Blood lipid control: hyperlipidemia can aggravate lipid deposition in the kidney and accelerate the progression of renal injury. Elderly patients with diabetes should regularly test their blood lipids to control their low density lipoprotein cholesterol (LDL-C) <2.6mmol/L. For patients with cardiovascular diseases, LDL-C should be controlled below 1.8mmol/L. In the selection of lipid-lowering agents, statins are preferred, with ezetimibe or PCSK9 inhibitors in combination if necessary.
04 Lifestyle intervention:
Dietary adjustment: Elderly patients with diabetic nephropathy should follow the principles of high-quality low-protein, low-sodium, low-fat and high-fiber diet. Protein intake should be controlled at 0.8g/kg body weight per day, which can be increased to 1.0-1.2g/kg per day in dialysis patients. At the same time, sodium intake should be limited, and the daily sodium intake should be less than 5g.
Moderate exercise: Moderate exercise helps control blood sugar, blood pressure and weight, and improves cardiovascular function. Elderly patients should choose gentle and easy to adhere to the type of exercise, such as walking, tai chi, gentle aerobics, etc., adhere to more than 5 times a week, about 30 minutes each time. Exercise time should avoid fasting and immediately after meals, and it is recommended to carry out 1-2 hours after meals.
Quit smoking and limit alcohol: smoking can aggravate oxidative stress and inflammatory response of the kidney, and accelerate the progress of kidney injury. Excessive alcohol consumption can affect glycemic control and increase the risk of cardiovascular disease. Therefore, elderly patients with diabetes should quit smoking and limit alcohol consumption.
Prevention and treatment of complications: Elderly patients with diabetic nephropathy are often complicated with cardiovascular disease, retinopathy, neuropathy and other complications, so the prevention and treatment of complications should be strengthened. Regular cardiovascular examination, fundus examination and neurological function examination were performed to detect and treat complications in time.
05 Psychological care: Elderly patients with diabetic nephropathy are prone to anxiety, depression and other psychological problems, these psychological problems will affect the patient’s treatment compliance and quality of life. Therefore, we should strengthen the psychological care of patients, help patients correctly understand the disease, build up confidence to overcome the disease.
5. Future prospects and challenges
In the context of aging, the prevention and control of diabetic nephropathy faces many challenges:
01 Uneven distribution of medical resources: There are a large number of elderly patients with diabetic nephropathy, but the medical resources are relatively insufficient, especially the diagnosis and treatment ability of primary medical institutions needs to be improved.
Limited cognitive level of patients: some elderly patients have insufficient knowledge of diabetic nephropathy and lack awareness of early screening and standardized treatment.
Imperfect multidisciplinary collaboration mechanism: The management of diabetic nephropathy requires the collaboration of endocrinology, nephrology, cardiology, nutrition and other multidisciplinary departments, but the multidisciplinary collaboration mechanism is not perfect at present. Insufficient research and development of innovative drugs and technologies: although some new hypoglycemic drugs and renal protective drugs have emerged in recent years, many patients still cannot obtain effective treatment. blood glucose meter at home
In the future, public health policy support should be strengthened and investment in the prevention and control of diabetic kidney disease should be increased. Improving the medical service system to enhance the diagnosis and treatment capacity of primary medical institutions; Strengthening health education to improve patients’ cognitive level and treatment compliance; Establishing a multidisciplinary collaboration mechanism to optimize the management model of diabetic nephropathy; The research and development of innovative drugs and technologies should be intensified to provide more treatment options for patients. Only in this way can we effectively deal with the crisis of diabetic nephropathy under the background of aging and protect the health rights of the elderly.
Post time: Mar-06-2026